Orthopedic conditions explained in simple terms
Also known as “disc prolapse” in medical terminology. Approximately one-third of all herniated discs occur in the cervical spine and approximately two-thirds in the lumbar spine. The most commonly affected disc segments are C5/6, L4/5, and L5/S1. Thirty percent of the total population is affected. The first symptoms can appear as early as age 20. The peak incidence is between the ages of 30 and 50. The prerequisite for the occurrence of a herniated disc is general wear and tear with tears in the fibrous ring of the disc (annulus fibrosus). A distinction is made between a prolapse (protrusion of disc tissue with perforation of the annulus fibrosus) and a protrusion (bulging with preservation of the annulus fibrosus). Accident-related destructio n of an intervertebral disc is very rare. The displaced disc tissue compresses individual or multiple nerve roots, causing pain and, in some cases, neurological deficits.
n of an intervertebral disc is very rare. The displaced disc tissue compresses individual or multiple nerve roots, causing pain and, in some cases, neurological deficits.
Therapy: Physiotherapy and manual therapy to strengthen the abdominal and back muscles, correct poor posture, and maintain mobility in the affected sections of the spine. Other measures include massage, heat applications (fango, red light, hot air), electrotherapy, targeted injections, and acupuncture. Elimination of excessive strain on the spine. Career counseling. No heavy physical activity, no heavy lifting or carrying of loads. Accompanying measures such as weight reduction and regular physical activity (fitness, swimming, yoga, rehabilitation sports).
Prognosis: The course of the disease is usually favorable, but treatment is relatively long (3–6 months on average). Spontaneous healing occurs through retraction of the prolapse and volume reduction due to scarring or displacement of the nerve root in the bony nerve canal. Severe forms (cauda syndrome, bladder and rectal disorders) are rare. Only in a few cases (less than 10%) is disc surgery necessary (nucleotomy, interlaminar fenestration, sequester removal, combination of dorsal disc removal, straightening and filling of the disc spaces, if necessary with stabilization, titanium cage interposition, insertion of an artificial disc).
Also referred to in medical terminology as a “popliteal cyst” or “synovial cyst.” This is a bulge of the knee joint capsule toward the back of the knee. The colloquial name refers to the first person to describe it, Dr. William Baker, a surgeon from London (1877). Damage to the meniscus or cartilage that persists for a long time is treated by the body itself. More joint fluid is produced to improve the sliding properties of the knee. However, if more joint fluid is produced than is broken down, this leads to knee joint effusion. If the increase in joint fluid continues for a long time, the joint capsule expands to make room for this effusion. The area where the knee joint capsule is least stable is the popliteal fossa.  Chronic excess pressure therefore causes a bulge in the popliteal fossa, known as a “Baker’s cyst.” The Baker’s cyst always causes discomfort when the pressure in the knee joint increases due to increased inflammatory activity or advanced cartilage damage. Surgical removal of the Baker’s cyst is not advisable if the cause—cartilage or meniscus damage—persists.
Chronic excess pressure therefore causes a bulge in the popliteal fossa, known as a “Baker’s cyst.” The Baker’s cyst always causes discomfort when the pressure in the knee joint increases due to increased inflammatory activity or advanced cartilage damage. Surgical removal of the Baker’s cyst is not advisable if the cause—cartilage or meniscus damage—persists.
Frequency: In principle, a Baker’s cyst can occur at any age. However, children are less frequently affected by cystic changes in the popliteal fossa. If a Baker’s cyst does develop in childhood, boys are twice as likely to be affected as girls. The condition is predominantly observed in middle and advanced age (45 to 60 years).
Therapy: Individual counseling covers everyday behavior, work, and sports (avoiding sports that put strain on the knees). Medication, intra-articular injections, physiotherapy, electrotherapy, wearing a knee brace to stabilize and improve joint function. Regular exercises to eliminate muscle deficits, strengthen the thigh muscles (cycling, swimming). The contents of the cyst can be sucked out with a puncture. However, recurrence of the cyst must be expected, as figuratively speaking, “the lake is pumped dry, but the river that feeds it continues to flow.” Conservative measures usually only lead to an improvement in the symptoms caused by the Baker’s cyst. The cyst is not expected to disappear or “dry up.” Only surgical treatment (knee arthroscopy, possibly with meniscus revision and cartilage smoothing) will cause the Baker’s cyst to disappear.
Also known medically as carpal tunnel syndrome (CTS), it is a chronic compression injury of the median nerve in the wrist. The nerve, along with other anatomical structures, is located in a narrow bony canal bordered by a ligament. The discrepancy between the canal’s volume and its contents leads to nerve compression. The extent of nerve damage depends primarily on the severity and duration of the compression. Between 3 and 5% of the population are affected. The female-to-male ratio is 2:1. A familial predisposition is observed.
 Possible causes: Malunited forearm fracture (distal radius fracture), dislocation of a carpal bone, wrist osteoarthritis with bone spur formation, rheumatic diseases of the joints and tendon sheaths, traumatic injuries (bruising, scarring, infection, bone fragments), tumors (wrist ganglion, neuromas), abnormal muscle development, hormonal changes during pregnancy, gigantism (acromegaly), metabolic disorders (diabetes, gout), thyroid dysfunction.
Possible causes: Malunited forearm fracture (distal radius fracture), dislocation of a carpal bone, wrist osteoarthritis with bone spur formation, rheumatic diseases of the joints and tendon sheaths, traumatic injuries (bruising, scarring, infection, bone fragments), tumors (wrist ganglion, neuromas), abnormal muscle development, hormonal changes during pregnancy, gigantism (acromegaly), metabolic disorders (diabetes, gout), thyroid dysfunction.
Symptoms: Primarily nocturnal sensory disturbances (“…my fingers go numb”), pain in the thumb, index and middle fingers, pain when holding objects, clumsiness and weakness of the hand, pain radiating into the forearm, difficulty with fine motor skills and pincer grasping (e.g., sewing, buttoning and unbuttoning, picking up and gripping objects), atrophy of the thenar muscles.
Therapy: Reduction and avoidance of overuse and improper strain in daily life, work, and sports. Further measures include: immobilization of the wrist in a forearm splint, wearing a wrist brace, injection of corticosteroids into the carpal tunnel to reduce swelling of the connective tissue, and acupuncture. During pregnancy, it is recommended to wait and see, depending on the symptoms and remaining duration of the pregnancy.
Prognosis: In most cases, surgery is necessary (resection of the flexor retinaculum or neurolysis of the median nerve). Open or endoscopic procedures are generally used. Pain and numbness usually subside rapidly after surgery. Muscle atrophy has a poorer prognosis. Relapses are rare.
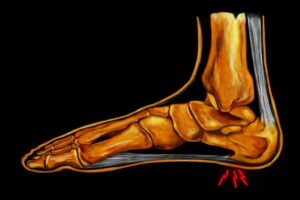
Also known in medical terminology as calcaneal periostitis or plantar fasciitis. The so-called heel spur is a thorn-like bony spur formation at the base of the tendon plate of the sole of the foot (plantar aponeurosis). However, it is often not a true bony protrusion, but rather a chronic inflammation that also involves the bursa on the heel bone. The cause is prolonged overuse of the foot, especially the large tendon plate under the sole of the foot. Overuse causes repeated small tears in the tendon. As with a broken bone, the body deposits calcium to heal the tears in the tendon. This often results in a bony protrusion in the area where the tendon plate attaches to the heel bone.
Symptoms: Pain during exertion usually develops gradually and rarely occurs suddenly. Typical for the initial phase is start-up pain (at the beginning of exertion, but also in the morning when getting up), which initially decreases with continued exertion. It can then develop into persistent pain, which becomes more pronounced with increasing exertion. Pain at rest can be triggered by stretching and tension against resistance. Localized pressure pain at the tendon attachment of the lower heel bone.
 Treatment: Reduction, avoidance of overexertion and incorrect strain in everyday life, work, and sports. Initially, gentle exercise, switching to sports that do not strain the affected heel region: e.g., cycling, swimming, etc. Local ice treatment, ultrasound, manual therapy in the area of the plantar tendon plate (transverse friction). Injection of corticosteroids into the painful area, wearing silicone heel cushions or shoe inserts with soft heel padding.
Treatment: Reduction, avoidance of overexertion and incorrect strain in everyday life, work, and sports. Initially, gentle exercise, switching to sports that do not strain the affected heel region: e.g., cycling, swimming, etc. Local ice treatment, ultrasound, manual therapy in the area of the plantar tendon plate (transverse friction). Injection of corticosteroids into the painful area, wearing silicone heel cushions or shoe inserts with soft heel padding.
Extracorporeal shock wave therapy (ESWT) has developed into a new, groundbreaking form of therapy in orthopedics in recent years. Shock waves are sound waves that are concentrated in a specific focal point (focus) where they take effect. ESWT reduces the activity of pain fibers, stimulates blood circulation, and reduces inflammation. This leads to rapid relief of symptoms and healing. There are no known side effects.
Prognosis: The course of the disease is usually favorable, with severe forms being rare. Once pain-free, it is essential to gradually and slowly build up stress. Sport-specific stress or partial stress can only be applied once it is possible without causing pain. Surgery is only a last resort, involving the severing of the tendon plate of the sole of the foot (plantar aponeurosis) and the removal of the bony heel spur.
This is a functional impairment of shoulder joint mobility. The rotator cuff of the shoulder joint is located in a narrow tendon canal bounded by the bony corner joint (acromion) and the head of the upper arm bone (humerus). The swollen tendons rub against each other when moving in this anatomically narrow space, causing inflammation and pain. Acute shoulder pain often occurs in younger and active patients. The main symptom is a dull, pulling pain in the deltoid muscle area. The arm hangs down from the body in a protective posture, and shoulder movements above 90° are hardly possible. Chronic shoulder pain leads to a protective posture and atrophy of the shoulder muscles.
 Diagnostic: typical examination findings with restricted shoulder mobility (“painful arc”). Ultrasound (sonography), X-ray to visualize bone structures or calcium deposits. The “gold standard” is magnetic resonance imaging (MRI). This allows ligaments, tendons, bursae, and especially the rotator cuff to be visualized.
Diagnostic: typical examination findings with restricted shoulder mobility (“painful arc”). Ultrasound (sonography), X-ray to visualize bone structures or calcium deposits. The “gold standard” is magnetic resonance imaging (MRI). This allows ligaments, tendons, bursae, and especially the rotator cuff to be visualized.
Treatment: Physiotherapy and manual therapy to strengthen the shoulder muscles and maintain mobility are the main components of treatment. In the acute stage, only targeted injection with an anti-inflammatory painkiller (corticosteroid) is usually helpful. Individual counseling covers everyday behavior, physical strain at work and in sports (avoiding overhead work, sports that place heavy strain on the shoulders).
Prognosis: The course of the disease is usually favorable, with severe forms being rare. Surgery (arthroscopy, possibly acromioplasty) is only necessary in isolated cases.
Also known as a meniscus tear in common parlance. A meniscus lesion is a disruption of the meniscus cartilage structure, degeneration of meniscus tissue, or a combination of both, with typical lesions associated with different ages. Menisci function as load distributors, brake pads, and shock absorbers for the knee joint. There is a smaller, crescent-shaped outer meniscus and a larger, sickle-shaped inner meniscus. Meniscus disease is caused by an accident (trauma) or general aging processes (degeneration). Meniscus damage reduces the load-bearing surface, increases pressure on the cartilage, and leads to increased wear and tear on the entire knee joint.
Trauma: Trauma occurs primarily in younger, active patients and requires movement of the joint beyond its normal range. The medial meniscus is firmly attached to the medial collateral ligament. The lateral meniscus is more mobile, lies on the outer tibial plateau, and follows the movement of the thigh better. It is less frequently affected by injuries.
Degeneration: The central two-thirds of the meniscus substance are nourished by synovial fluid, while the third closest to the capsule is supplied with blood vessels. The transition zone between the two areas is also the most common site for longitudinal tears. Pre-damaged menisci can tear even during normal knee movements.
 Therapy: Individual counseling covers behavior in everyday life, at work, and during sports (avoiding deep squats and sports involving rapid changes of direction). Medication, intra-articular injections, physiotherapy (mobilization, muscle stretching techniques), electrotherapy, wearing a knee brace to stabilize and improve joint function. Regular exercises to eliminate muscle deficits and strengthen the thigh muscles.
Therapy: Individual counseling covers behavior in everyday life, at work, and during sports (avoiding deep squats and sports involving rapid changes of direction). Medication, intra-articular injections, physiotherapy (mobilization, muscle stretching techniques), electrotherapy, wearing a knee brace to stabilize and improve joint function. Regular exercises to eliminate muscle deficits and strengthen the thigh muscles.
Arthroskopy: Partial removal of a meniscus serves to relieve pain by removing all damaged and mobile parts of the meniscus. As much “healthy” meniscus tissue as possible is preserved during this procedure. Knee arthroscopy is performed as an outpatient procedure under local or general anesthesia. The surgical procedure depends on the shape and location of the tear: All mobile fragments are removed, the resection margin is smoothed, a rim and the connection to the capsule are left in place, and the joint is rinsed.
Also commonly referred to as “round back” or “apprentice’s hump.” This is a growth disorder that occurs in adolescence in the area of the base and cover plates of the thoracic and/or lumbar spine, with increased rounding of the back (juvenile kyphosis). The cause of Scheuermann’s disease is unknown. A familial clustering with autosomal dominant inheritance is reported. Mechanical and genetic factors with reduced load-bearing capacity of the vertebral bodies, changes in the vertebral body margins, vitamin deficiency syndromes, etc. may play a role. Disc protrusions into the spongy vertebral body parts (Schmorl’s nodes) are the typical signs of the disease on X-rays. Severe cases are rare, but they can result in wedge-shaped vertebrae. 10% of the total population is affected. Scheuermann’s disease is the most common disease in adolescence (20%). The first physical symptoms can appear as early as age 10. The peak incidence of the disease is between the ages of 12 and 16. The male to female ratio is 2:1.
 The changes to the vertebrae that are typical of the disease stabilize once growth is complete. Other pain syndromes caused by spinal misalignment can also occur later in life.
The changes to the vertebrae that are typical of the disease stabilize once growth is complete. Other pain syndromes caused by spinal misalignment can also occur later in life.
Therapy: Physiotherapy and manual therapy to strengthen the back muscles and maintain mobility in the affected sections of the spine. Other measures include heat treatments (hot air, red light, fango), massages, electrotherapy, TENS, and acupuncture. Accompanying medication (muscle relaxants, anti-inflammatory painkillers). Elimination of excessive strain on the spine. Career counseling. No heavy physical activity, no heavy lifting or carrying of loads. Accompanying measures such as weight reduction, training of the abdominal and back muscles, regular physical activity (fitness, gymnastics, back training, swimming).
Prognosis: The course of the disease is benign, and severe forms are rare. Only in severe cases during puberty is a corset sometimes required (for curvatures of 45 degrees or more: Milwaukee or Boston corset) or surgery (fixed kyphosis in a fully grown skeleton at an angle of 60 degrees or more, combination of ventral disc removal, straightening and filling of the disc spaces with the patient’s own bone with dorsal stabilization) is sometimes necessary.
Also commonly referred to as “spinal curvature” or “lateral curvature.” This is a curvature of one or more sections of the spine, accompanied by a twist (torsion) and partial stiffening of the vertebrae. It is a growth disorder of the spine that occurs during adolescence. The cause of scoliosis is unknown. However, retrospective studies and twin studies have shown a familial clustering without evidence of a hereditary mechanism. Genetic or mechanical factors with reduced spinal load-bearing capacity, adhesions from accidents, vertebral bodies, nerve disorders, and leg length differences may play a role. 10-15% of the total population is affected. Scoliosis is the most common disease in puberty (30%). The first physical symptoms can appear as early as age 10, with the peak incidence between ages 12 and 15. The gender ratio is female : male = 3 : 1.
 The characteristic curvature of the spine can be recognized by a rib hump and lumbar bulge. Other pain syndromes in the thoracic or lumbar spine can also occur in adulthood.
The characteristic curvature of the spine can be recognized by a rib hump and lumbar bulge. Other pain syndromes in the thoracic or lumbar spine can also occur in adulthood.
Therapy: Physiotherapy and manual therapy to strengthen the back muscles and correct the misalignment of the affected sections of the spine are the main components of the treatment. Other measures include electrostimulation, compensation for any leg length differences, and massage. Elimination of excessive strain on the spine. Consideration when choosing a career. No heavy physical activity. Regular exercise, e.g., fitness, gymnastics, swimming.
Prognosis: The course of the disease is usually favorable, with severe forms being rare. Scoliosis requires regular medical checkups and intensive, long-term treatment. Only in isolated cases is a corset (Milwaukee or Boston corset) or, if necessary, surgery (fixed scoliosis with an angle of 40° or more, combination of ventral disc removal, straightening, and filling of the disc spaces with the patient’s own bone with ventral or dorsal stabilization) necessary. Once growth is complete, there is usually no significant deterioration in the findings.
Also known as slipping vertebral bone in common parlance. This refers to the forward slippage of a vertebral body with its arcuate roots, transverse processes, and superior articular processes (and thus also with the vertebra above it) over the next lower vertebra. The incidence in the general population is 4-8%. It is more common in athletes who place heavy strain on the lumbar spine (javelin throwers 50%, judokas, gymnasts, wrestlers 25%). In 80% of all patients, the 5th lumbar vertebra is affected (segment L5/S1), and in 15% the 4th lumbar vertebra (segment L4/L5). A prerequisite for true spondylolisthesis is a gap formation (spondylolysis) in the area of the vertebral arch (5-7% of Caucasians, most common in Eskimos at 40%). Spondylolysis can develop due to malformation of the vertebral arch (genetic factors), after an accident, or as a fatigue fracture. It is often combined with transitional disorders, e.g., an incompletely closed vertebral arch (spina bifida). Classification according to the severity of spondylolisthesis Grades 1-4 according to Meyerding.
 Therapy: Pain relief or reduction. Prevention of increased vertebral slippage. Elimination of any neurological symptoms. Physiotherapy and manual therapy to strengthen the abdominal and back muscles and maintain mobility in the affected sections of the spine. Other treatment measures include heat applications (hot air, fango), massages, extensions, electrotherapy, TENS, or acupuncture. Elimination of excessive strain on the spine. Career counseling, no heavy lifting or carrying of loads. Avoidance of stooped activities or compressive loads. Accompanying measures such as weight reduction and regular physical activity.
Therapy: Pain relief or reduction. Prevention of increased vertebral slippage. Elimination of any neurological symptoms. Physiotherapy and manual therapy to strengthen the abdominal and back muscles and maintain mobility in the affected sections of the spine. Other treatment measures include heat applications (hot air, fango), massages, extensions, electrotherapy, TENS, or acupuncture. Elimination of excessive strain on the spine. Career counseling, no heavy lifting or carrying of loads. Avoidance of stooped activities or compressive loads. Accompanying measures such as weight reduction and regular physical activity.
Prognosis: The course of the disease is usually favorable, with severe forms being rare. The slippage process can come to a spontaneous halt at any stage. As the slippage increases, so does the likelihood of symptoms, functional disorders, or neurological symptoms occurring. Prescription of aids (corset, girdle, lumbar bandage). Surgery is only necessary in isolated cases (instrumented spinal fusion, known as spondylodesis, with or without reduction; internal fixator; interbody metal implants; bone grafting; dorsal, ventral, or ventrodorsal surgical procedures).